The Iliotibial Band (ITB) is a common source of knee pain that we see commonly in clinic. It is due to inflammation of the distal portion of the iliotibial band, and this results in pain that occurs around the outside portion of the knee. The repetitive bending and straightening of the knee with daily activities such as walking or running can lead to potential irritation of certain portions of the IT band that eventually can lead to injury.
ITB syndrome is one of the most common injuries in runners presenting with lateral knee pain, with an incidence estimated to between 5% and 14%. Further studies indicate that ITBS is responsible for approximately 22% of all lower extremity injuries.
Long distance running is a common cause of ITB pain, especially if running on slightly banked ground, as the subtle drop of the outside of the foot stretches the ITB, increasing the risk of injury, Sudden increases in activity levels can also lead to ITB syndrome. Although repeated tissue compression leading to irritation is best supported by recent evidence, there are a number of other trains of thought regarding the evolution of this condition.
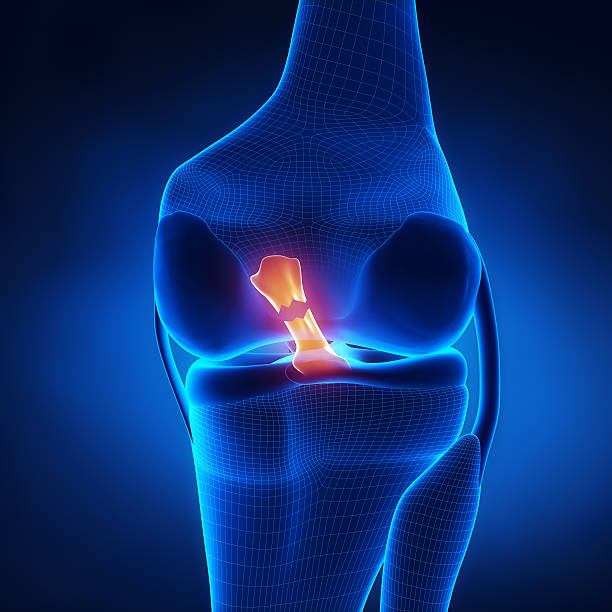
When the knee is positioned in extension the iliotibial band lies anterior to the lateral femoral epicondyle. When the knee is positioned in 30° of flexion the band moves posteriorly to the lateral femoral epicondyle. It is hypothesised that friction can therefore occur between the posterior edge of the iliotibial band and the underlying lateral femoral epicondyle.
Muscle weakness of the hip abductors is also be associated with iliotibial band syndrome as this causes increased hip internal rotation and knee adduction. This was found as a significant issue for athletes with iliotibial band syndrome.
ANATOMY OF THE ITB
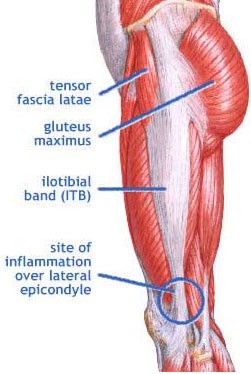
The iliotibial band is a thick band of fascia formed proximally at the hip by the fascia of the gluteus maximus, gluteus meduis and tensor fasciae latae muscles.
It traverses superficial to the vastus lateralis and inserts on the Gerdy tubercle of the lateral tibial plateau and partially to the supracondylar ridge of the lateral femur. There is also an anterior extension called the iliopatella band that connects the lateral patella and prevents medial translation of the patella.
A small recess exists between the lateral femoral epicondyle and the ITB, which contains a synovial extension of the knee joint capsule (lateral synovial recess)
The ITB shares the innervation of the TFL and gluteus maximums via the superior gluteal nerve and inferior gluteal nerve.
Composition: The Iliotibial Band is made up of mostly collagen fibers. Collagen is the strongest protein found in nature. The collagen fibres are aligned in a very organized, vertical fashion as this allows for better force absorption with weight bearing activities. There is a small amount of elastin fibers amongst the layers of collagen, which allow it to be slightly elastic and pliable helping it act as a spring. However, this does not give it the ability to stretch like a muscle. What is unique about the iliotibial band is the type of tissue that it is- the iliotibial band is a type of connective tissue; however, its properties are different than tissue such as muscle, tendon, or ligaments.
In contrast to tissues such as muscles, tendons, and ligaments, the iliotibial band itself does NOT perform actual contractions within the human body! This is a very important concept to understand when one is conceptualizing the anatomical and physiological properties of the IT band. Furthermore, when one is overcoming an IT band origin of pain, the underlying origin of the source of pain may not be the IT band itself, but the muscular attachments that connect to the IT band.
The Movement Perfected Team are trained to assess, treat and rehabilitate ITB injuries.
The major goals of treating and rehabilitation of the iliotibial band are:
– Gain full ROM of the knee
– Decrease inflammation
– Repair muscle strength and proprioception
– Gain good functional stability
– Reach the best possible functional level (walking, running, jumping)
– Decrease the risk for re-injury
– (Return to sport)
Click here to book appointment